Clinical Overview
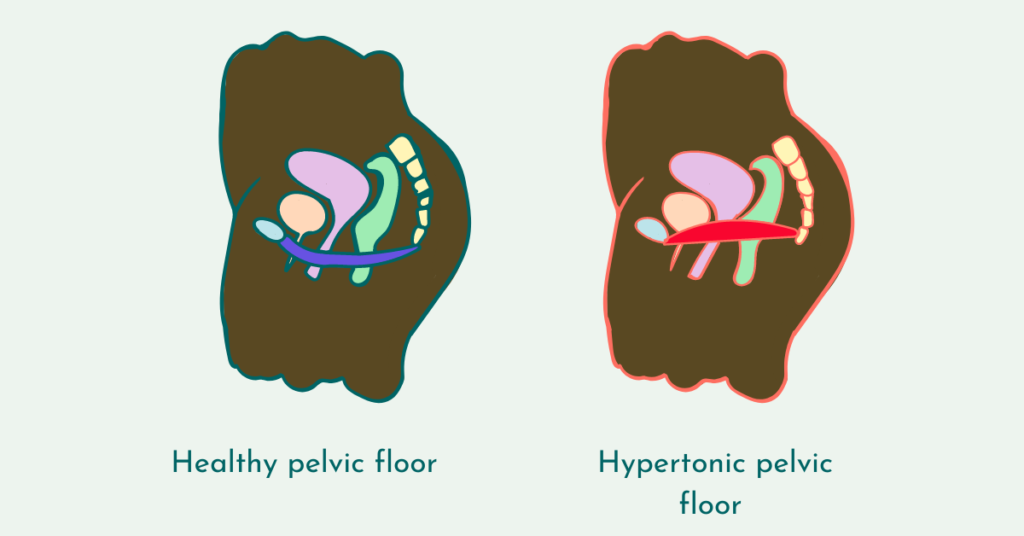
A hypertonic pelvic floor, also known as an overactive pelvic floor, occurs when the pelvic floor muscles remain in a constant state of contraction rather than relaxing appropriately.
Unlike pelvic floor weakness, this condition is characterised by excess muscle tension, which can lead to pain, dysfunction, and difficulty with normal bodily functions such as urination, bowel movements, and sexual activity.
The pelvic floor must be able to both contract and relax. When relaxation is impaired, normal function is disrupted.
What Causes a Hypertonic Pelvic Floor?
This condition is typically multifactorial and may involve physical, neurological, and psychological contributors.
Muscle Overactivity
- Chronic clenching or guarding of pelvic muscles
- Overtraining (excessive or incorrect Kegel exercises)
Nervous System Dysregulation
- Increased sympathetic (stress) response
- Reduced ability to down-regulate muscle tone
Pain or Trauma
- Previous painful experiences (e.g. intercourse, medical procedures)
- Childbirth trauma
- Injury or surgery
Associated Medical Conditions
- Vaginismus
- Endometriosis
- Interstitial cystitis
- Irritable bowel syndrome (IBS)
Symptoms
Symptoms often reflect the inability of the pelvic floor to relax.
Pain-Related Symptoms
- Pain with penetration (dyspareunia)
- Burning, aching, or tightness in the pelvic region
- Pain when sitting for extended periods
Urinary Symptoms
- Difficulty starting urine flow
- Feeling of incomplete emptying
- Urinary urgency without infection
Bowel Symptoms
- Constipation
- Straining or incomplete evacuation
Sexual Function Symptoms
- Difficulty inserting tampons or undergoing examinations
- Reduced comfort or avoidance of intimacy
Pathophysiology (What’s Happening in the Body)
A hypertonic pelvic floor involves:
- Increased resting muscle tone
- Reduced blood flow to the area
- Heightened nerve sensitivity (central sensitisation)
- Trigger points within the pelvic muscles
Over time, this can create a pain-tension cycle, where pain leads to more muscle guarding, which further increases pain.

Clinical Assessment
A proper diagnosis involves identifying both physical and contributing factors.
1. Subjective Assessment
- Pain history
- Triggers and patterns
- Psychological or stress-related factors
2. Physical Examination
- Assessment of resting muscle tone
- Identification of trigger points
- Evaluation of relaxation ability
3. Functional Assessment
- Coordination between contraction and relaxation
- Breathing pattern assessment
Evidence-Based Treatment Approach
Treatment focuses on reducing muscle tension and restoring normal function, not strengthening.
Phase 1: Downtraining & Nervous System Regulation
Goal: Reduce baseline muscle tension
- Diaphragmatic breathing (deep abdominal breathing)
- Relaxation techniques (guided or self-directed)
- Stress management strategies
This phase is critical and often overlooked.
Phase 2: Pelvic Floor Relaxation Training
Goal: Restore the ability to relax the pelvic floor
- Focus on “letting go” rather than contracting
- Visualisation techniques (e.g. dropping or lengthening the pelvic floor)
- Coordination with breathing
Phase 3: Desensitisation & Graded Exposure
Goal: Reduce pain and improve tolerance
- Introduction of small-size dilators
- Gentle, passive insertion only
- No force or discomfort
Sessions should focus on comfort and control, not progression speed.
Phase 4: Gradual Progression
Goal: Improve flexibility and function
- Progress through dilator sizes slowly
- Maintain relaxed breathing throughout
- Only progress when completely comfortable
Phase 5: Functional Reintegration
Goal: Return to normal activity
- Reintroduce pain-free sexual activity
- Improve tolerance for sitting, movement, and daily tasks
- Address contributing lifestyle factors
Common Mistakes
- Performing Kegel exercises (which can worsen the condition)
- Rushing dilator progression
- Ignoring the role of stress and the nervous system
- Forcing insertion or pushing through pain
- Skipping relaxation training
Where Therapeutic Support Can Help
When used correctly, therapeutic tools can assist in treatment:
-
Graduated dilator sets
→ Allow controlled, step-by-step desensitisation -
Water-based lubricants
→ Reduce friction and discomfort during therapy -
Antibacterial cleaners
→ Maintain hygiene and reduce irritation risk
These tools should always be used within a relaxation-focused protocol, not a strengthening approach.
Explore Structured dilator therapy kits designed for gradual, guided pelvic floor relaxation
Expected Recovery Timeline
| Timeframe | What to Expect |
|---|---|
| 2–4 weeks | Improved awareness and reduced tension |
| 4–8 weeks | Decreased pain and improved tolerance |
| 2–4 months | Gradual return to normal function |
| 4–6 months | Significant symptom improvement (varies) |
Consistency and a gentle approach are key.
When to Seek Professional Help
Consult a healthcare professional if you experience:
- Persistent pelvic pain
- Severe pain with penetration
- No improvement with relaxation techniques
- Significant impact on quality of life
Pelvic floor physiotherapy is often highly effective for this condition.
Summary
A hypertonic pelvic floor is a common but often misunderstood condition. Unlike weakness, it requires relaxation, not strengthening.
With the correct approach, focused on downtraining, desensitisation, and gradual progression, most individuals can achieve significant improvement.